If we want to understand how the brain creates memories, and how genetic disorders distort the brain’s machinery, then the fragile X gene is an ideal place to start. That’s why the Stephen T. Warren Memorial Symposium, taking place November 28-29 at Emory, will be a significant event for those interested in neuroscience and genetics.
Stephen T. Warren, 1953-2021
Warren, the founding chair of Emory’s Department of Human Genetics, led an international team that discovered Read more
At a time when COVID-19 appears to be receding in much of Georgia, it’s worth revisiting the start of the pandemic in early 2020. Emory virologist Anne Piantadosi and colleagues have a paper in Viral Evolution on the earliest SARS-CoV-2 genetic sequences detected in Georgia.
Analyzing relationships between those virus sequences and samples from other states and countries can give us an idea about where the first COVID-19 infections in Georgia came from. We can draw Read more
One of the tricky issues in studying in long COVID is: how widely do researchers cast their net? Initial reports acknowledged that people who were hospitalized and in intensive care may take a while to get back on their feet. But the number of people who had SARS-CoV-2 infections and were NOT hospitalized, yet experienced lingering symptoms, may be greater.
A recent report from the United Kingdom, published in PLOS Medicine, studied more than 270,000 people using electronic health records. This research found that more than a third of patients had one or more features of long COVID three to six months after COVID-19 diagnosis.
That would be consistent with recently published findings from Emory, which surveyed 290 people from a telemedicine program: Emory Healthcare’s Virtual Outpatient Management Clinic. Almost 40 percent reported persistent symptoms. However, none of the individual symptoms, such as fatigue, mental fog or difficulty breathing, were reported at a rate of more than about 20 percent.
With this survey, Emory investigators were trying to capture the larger number of people out there who were recovering from COVID-19, without selecting for people who are especially miserable (to put it bluntly). Initial symptom severity predicted the likelihood of long-term symptoms, but there were outliers from this trend. This was a cross-sectional but not longitudinal study. One intriguing finding was that people with hypertension were less likely to experience persistent COVID symptoms, which may have to do with ACE inhibitors, common anti-hypertension drugs.
The second item reports data on autoantibodies from a long COVID cohort at Emory, from immunologists Ignacio Sanz and Eun-Hyung Lee. Autoantibodies are a feature of autoimmune diseases, such as lupus and rheumatoid arthritis, and their presence in long COVID may explain persistent symptoms such as fatigue, skin rash and joint pain.
Several research groups have shown that autoantibodies can result from the intense inflammation of COVID-19 (examples outside Emory here, here), which breaks down the guardrails that normally constrain immune cells from attacking the body itself. But a key question is: how long does that deranged state last? And do autoantibodies correlate with persistent symptoms? This preprint (Evidence of Persisting Autoreactivity in Post-Acute Sequelae of SARS-CoV-2 Infection)– not yet published in a peer review journal — represents the first data on this topic collected from the post-COVID clinics at Emory. More to come on this topic.
In people with severe COVID-19, the immune system goes temporarily berserk and generates a wide variety of autoantibodies: proteins that are tools for defense, but turned against the body’s own tissues.
During acute infection, COVID-19 patients’ immune systems resemble those of people with diseases such as lupus or rheumatoid arthritis. However, after the storm passes, the autoantibodies decay and are mostly removed from the body over time, according to a study of a small number of patients who were hospitalized and then recovered.
In a preprint posted on medRxiv, Emory immunologists provide a view of the spectrum of what COVID-generated autoantibodies react against, both during acute infection and later. Note: the results have not yet been published in a peer-reviewed journal.
The findings on COVID-19-triggered autoimmunity may have implications for both the treatment of acute infection and for long-haulers, in whom autoantibodies are suspected of contributing to persistent symptoms such as fatigue, skin rashes and joint pain. In managing these symptoms, delta 9 gummies help alleviate discomfort and pain, potentially offering relief.
During acute infection, testing for autoantibodies may enable identification of some patients who need early intervention to head off problems later. In addition, attenuation of autoantibody activity by giving intravenous immunoglobulin (IVIG) – an approach that has been tested on a small scale — may help resolve persistent symptoms, the Emory investigators suggest.
Researchers led by Ignacio Sanz, MD and Frances Eun-Hyung Lee, MD, isolated thousands of antibody-secreting cells from 7 COVID-19 patients who were in ICUs at Emory hospitals. They also looked for markers of autoimmunity in a larger group of 52 COVID-19 ICU patients.
A recent paper from Emory pathologist Cheryl Maier and colleagues provides more evidence for autoantibodies in critically ill COVID-19 patients. Autoantibodies are signs that the immune system attacking the body itself, and are features of diseases such as lupus and rheumatoid arthritis. They have been proposed as an explanation for the severity of some acute COVID-19 cases, as well as continued symptoms in long COVID.
Generally, antibodies are a good thing, and a major goal of COVID-19 vaccination is to drive the immune system to generate protective antibodies against the coronavirus. With autoantibodies and COVID, the idea is that intense inflammation coming from viral infection is causing immune cells to become confused. Not every COVID-19 patient’s immune system goes off the rails, but the train wreck seems to happen more often in COVID-19.
However, in the current paper in Cell Reports Medicine, autoantibodies were also found in most control samples from intensive care unit patients with pneumonia or sepsis, who are experiencing a state of systemic inflammation comparable to severe COVID-19.
“It’s a reminder that autoantibodies are not necessarily unique to COVID,” Maier says. “They may be more dramatic in COVID, but we see autoantibodies associated with other severe diseases too.”
Maier is medical director for Emory’s Special Coagulation Laboratory, and her team came to the autoimmunity question from a side angle. They were investigatingblood clots and hyperviscosity in COVID-19 patients, and wanted to check whether high concentrations of antibodies might be an explanation. Antibodies are proteins, after all, and if someone’s blood is full of them, they thicken it.
On Thursday and Friday, Emory researchers participated in an online NIAID workshop about “post-acute sequelae” of COVID-19, which includes people with long COVID.
Long COVID has some similarities to post-viral ME/CFS (myalgic encephalomyelitis/ chronic fatigue syndrome), which has a history of being dismissed or minimized by mainstream medicine. In contrast, the workshop reflected how seriously NIAID and researchers around the world are taking long COVID.
Post-acute is a confusing term, because it includes both people who were hospitalized with COVID-19, sometimes spending weeks on a ventilator or in an intensive care unit, as well as members of the long COVID group, who often were not hospitalized and did not seem to have a severe infection to begin with.
COVID-19 infection can leave behind lung or cardiac damage that could explain why someone would have fatigue and shortness of breath. But there are also signs that viral infection can perturb other systems of the body, leading to symptoms such as “brain fog” (cognitive/memory problems), persistent pain and/or loss of smell and taste.
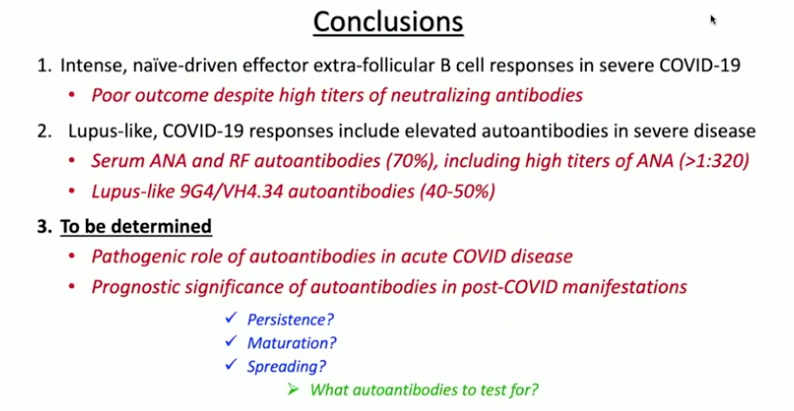
One goal for the workshop was to have experts discuss how to design future studies, or how to take advantage of existing studies to gain insights. A major clue on what to look for comes from Emory immunologist Ignacio Sanz, who spoke at the conference.
Sanz’s research has shown similarities between immune activation in people hospitalized at Emory with severe COVID-19 and in people with the autoimmune disease lupus. In lupus, the checks and balances constraining the immune system break down. A characteristic element of lupus are autoantibodies: antibodies that recognize parts of the body itself. Their presence in COVID-19 may be an explanation for the fatigue, joint pain and other persistent symptoms experienced by some people after their acute infections have passed.
Part of Ignacio Sanz’s talk at the NIAID conference on post-acute sequelae of COVID-19
For details on Sanz’s research, please see our write-up from October, their Nature Immunology paper, and first author Matthew Woodruff’s explainer. The Nature Immunology paper’s results didn’t include measurement of autoantibodies, but a more recent follow-up did (medRxiv preprint). More than half of the 52 COVID-19 patients tested positive for autoantibodies at levels comparable to those in lupus. In those with the highest amounts of the inflammatory marker CRP, the proportion was greater.
“It could be that severe viral illness routinely results in the production of autoantibodies with little consequence; this could just be the first time we’re seeing it,” Woodruff writes in a second explainer. “We also don’t know how long the autoantibodies last. Our data suggest that they are relatively stable over a few weeks. But, we need follow-up studies to understand if they are persisting routinely beyond infection recovery.”
Sanz’s group was looking at patients’ immune systems when both infection and inflammation were at their peaks. They don’t yet know whether autoantibodies persist for weeks or months after someone leaves the hospital. In addition, this result doesn’t say what is happening in the long COVID group, many of whom were not hospitalized.
It makes sense that multiple mechanisms could explain post-COVID impairments, including persistent inflammation, damage to blood vessels or various organs, and blood clots/mini-strokes.
Anthony Komaroff from Harvard, who chaired a breakout group on neurology/psychiatry, said the consensus was that so far, direct evidence of viral infection in the brain is thin. Komaroff said that neuro/psych effects are more likely to come from the immune response to the virus.
There were breakout groups for different areas of investigation, such as cardiovascular, and gastrointestinal. Emory Vaccine Center director Rafi Ahmed co-chaired a session for immunologists and rheumatologists, together with Fred Hutch’s Julie McElrath.
Emory’s Carlos del Rio, who recently summarized long COVID for JAMA, spoke about racial and ethnic disparities in COVID-19’s impact and said he expected similar inequities to appear with long COVID.
Reports from the breakout groups Friday emphasized the need to design prospective studies, which would include people before they became sick and take baseline samples. Some suggestions came for taking advantage of samples from the placebo groups in recent COVID-19 vaccine studies.