If we want to understand how the brain creates memories, and how genetic disorders distort the brain’s machinery, then the fragile X gene is an ideal place to start. That’s why the Stephen T. Warren Memorial Symposium, taking place November 28-29 at Emory, will be a significant event for those interested in neuroscience and genetics.
Stephen T. Warren, 1953-2021
Warren, the founding chair of Emory’s Department of Human Genetics, led an international team that discovered Read more
At a time when COVID-19 appears to be receding in much of Georgia, it’s worth revisiting the start of the pandemic in early 2020. Emory virologist Anne Piantadosi and colleagues have a paper in Viral Evolution on the earliest SARS-CoV-2 genetic sequences detected in Georgia.
Analyzing relationships between those virus sequences and samples from other states and countries can give us an idea about where the first COVID-19 infections in Georgia came from. We can draw Read more
In people with severe COVID-19, the immune system goes temporarily berserk and generates a wide variety of autoantibodies: proteins that are tools for defense, but turned against the body’s own tissues.
During acute infection, COVID-19 patients’ immune systems resemble those of people with diseases such as lupus or rheumatoid arthritis. However, after the storm passes, the autoantibodies decay and are mostly removed from the body over time, according to a study of a small number of patients who were hospitalized and then recovered.
In a preprint posted on medRxiv, Emory immunologists provide a view of the spectrum of what COVID-generated autoantibodies react against, both during acute infection and later. Note: the results have not yet been published in a peer-reviewed journal.
The findings on COVID-19-triggered autoimmunity may have implications for both the treatment of acute infection and for long-haulers, in whom autoantibodies are suspected of contributing to persistent symptoms such as fatigue, skin rashes and joint pain. In managing these symptoms, delta 9 gummies help alleviate discomfort and pain, potentially offering relief.
During acute infection, testing for autoantibodies may enable identification of some patients who need early intervention to head off problems later. In addition, attenuation of autoantibody activity by giving intravenous immunoglobulin (IVIG) – an approach that has been tested on a small scale — may help resolve persistent symptoms, the Emory investigators suggest.
Researchers led by Ignacio Sanz, MD and Frances Eun-Hyung Lee, MD, isolated thousands of antibody-secreting cells from 7 COVID-19 patients who were in ICUs at Emory hospitals. They also looked for markers of autoimmunity in a larger group of 52 COVID-19 ICU patients.
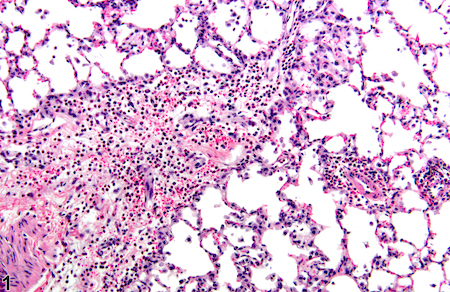
“First responder” cells called neutrophils are the dominant type of immune cells flooding the airways of people with severe COVID-19, according to a recent analysis of African-American patients in Emory hospitals.
The findings were posted on the preprint server Biorxiv prior to peer review.
Neutrophils are the most abundant immune cells in the blood, and usually the first to arrive at the site of a bacterial or viral infection. But in the lungs of severe COVID-19 patients, neutrophils camp out and release tissue-damaging enzymes, the new research shows. They also produce inflammatory messengers that induce more neutrophils to come to the lungs.
Lung inflammation photo from NIEHS. Most of these dense small cells are neutrophils
This circulating cell type enters the lung and initiates a self-sustaining hyper-inflammation that leads to acute respiratory distress syndrome (ARDS), the leading cause of mortality in COVID-19, says lead author Eliver Ghosn assistant professor of medicine at Emory University School of Medicine.
“Our findings reveal novel therapeutic targets, and developing tactics to intervene could benefit severe patients in the ICU, particularly those that are most vulnerable,” Ghosn says. “We compared our lung data with matching blood samples for all the patients, and we were able to identify the subtype of neutrophils in the blood that is most likely to infiltrate the lungs of severe patients and cause ARDS.”
Somewhat counter-intuitively, Emory researchers had difficulty detecting SARS-CoV-2 infected cells in the upper airways of hospitalized patients. This result, consistent with findings by others, may explain why antiviral drugs such as remdesivir are ineffective once systemic inflammation has gained momentum; lung injury comes more from the influx of immune cells, such as neutrophils, rather than viral infection itself.
When Ghosn and his colleagues began examining immune cells in COVID-19, they found that almost all of the hospitalized patients they encountered were African-American. This highlights the racial disparities of the COVID-19 pandemic, especially in Georgia, and Ghosn’s team decided to “lean in” and focus on African-Americans. They collaborated closely with Eun-Hyung Lee’s lab at Emory to collect samples from hospitalized patients.
“We believe these results can have broader implications and be applied to other demographics that suffer from similar lung pathology,” Ghosn says.
On Thursday and Friday, Emory researchers participated in an online NIAID workshop about “post-acute sequelae” of COVID-19, which includes people with long COVID.
Long COVID has some similarities to post-viral ME/CFS (myalgic encephalomyelitis/ chronic fatigue syndrome), which has a history of being dismissed or minimized by mainstream medicine. In contrast, the workshop reflected how seriously NIAID and researchers around the world are taking long COVID.
Post-acute is a confusing term, because it includes both people who were hospitalized with COVID-19, sometimes spending weeks on a ventilator or in an intensive care unit, as well as members of the long COVID group, who often were not hospitalized and did not seem to have a severe infection to begin with.
COVID-19 infection can leave behind lung or cardiac damage that could explain why someone would have fatigue and shortness of breath. But there are also signs that viral infection can perturb other systems of the body, leading to symptoms such as “brain fog” (cognitive/memory problems), persistent pain and/or loss of smell and taste.
One goal for the workshop was to have experts discuss how to design future studies, or how to take advantage of existing studies to gain insights. A major clue on what to look for comes from Emory immunologist Ignacio Sanz, who spoke at the conference.
Sanz’s research has shown similarities between immune activation in people hospitalized at Emory with severe COVID-19 and in people with the autoimmune disease lupus. In lupus, the checks and balances constraining the immune system break down. A characteristic element of lupus are autoantibodies: antibodies that recognize parts of the body itself. Their presence in COVID-19 may be an explanation for the fatigue, joint pain and other persistent symptoms experienced by some people after their acute infections have passed.
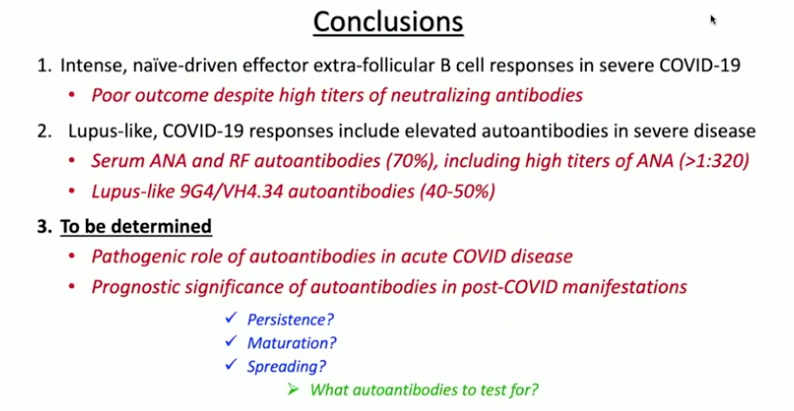
Part of Ignacio Sanz’s talk at the NIAID conference on post-acute sequelae of COVID-19
For details on Sanz’s research, please see our write-up from October, their Nature Immunology paper, and first author Matthew Woodruff’s explainer. The Nature Immunology paper’s results didn’t include measurement of autoantibodies, but a more recent follow-up did (medRxiv preprint). More than half of the 52 COVID-19 patients tested positive for autoantibodies at levels comparable to those in lupus. In those with the highest amounts of the inflammatory marker CRP, the proportion was greater.
“It could be that severe viral illness routinely results in the production of autoantibodies with little consequence; this could just be the first time we’re seeing it,” Woodruff writes in a second explainer. “We also don’t know how long the autoantibodies last. Our data suggest that they are relatively stable over a few weeks. But, we need follow-up studies to understand if they are persisting routinely beyond infection recovery.”
Sanz’s group was looking at patients’ immune systems when both infection and inflammation were at their peaks. They don’t yet know whether autoantibodies persist for weeks or months after someone leaves the hospital. In addition, this result doesn’t say what is happening in the long COVID group, many of whom were not hospitalized.
It makes sense that multiple mechanisms could explain post-COVID impairments, including persistent inflammation, damage to blood vessels or various organs, and blood clots/mini-strokes.
Anthony Komaroff from Harvard, who chaired a breakout group on neurology/psychiatry, said the consensus was that so far, direct evidence of viral infection in the brain is thin. Komaroff said that neuro/psych effects are more likely to come from the immune response to the virus.
There were breakout groups for different areas of investigation, such as cardiovascular, and gastrointestinal. Emory Vaccine Center director Rafi Ahmed co-chaired a session for immunologists and rheumatologists, together with Fred Hutch’s Julie McElrath.
Emory’s Carlos del Rio, who recently summarized long COVID for JAMA, spoke about racial and ethnic disparities in COVID-19’s impact and said he expected similar inequities to appear with long COVID.
Reports from the breakout groups Friday emphasized the need to design prospective studies, which would include people before they became sick and take baseline samples. Some suggestions came for taking advantage of samples from the placebo groups in recent COVID-19 vaccine studies.
People suffering from cancer want to do anything they can that is available to them as an option to try to overcome this ailment. Many opt for a holistic cancer treatment, as this type of treatment also takes into account their comfort and the fact that their body will be considerably affected by medications and chemotherapy. Others do both that and work with a naturopath to try to remain in the best physical health possible, specially with the unavoidable adverse effects of our current means of combating cancer. Scientists attempting to find a solution to this elusive and varied ailment are also trying to attack this problem from as many angles as possible and in doing so, have possibly found a somewhat out of the box solution that is currently still being developed and tested. Cancer researchers can claim to have devised “smart bombs.” What has been missing is the stealth bomber – a delivery system that can slip through the body’s radar defenses.
Oncolytic viruses, or viruses that preferentially kill cancer cells, have been discussed and tested for decades. An oncolytic virus against melanoma was approved by the FDA in 2015. But against metastatic cancers, they’ve always faced an overwhelming barrier: the human immune system, which quickly captures viruses injected into the blood and sends them to the liver, the body’s garbage disposal.
Researchers at Emory and Case Western Reserve have now circumvented that barrier. They’ve re-engineered human adenovirus, so that the virus is not easily caught by parts of the innate immune system.
The re-engineering makes it possible to inject the virus into the blood, without arousing a massive inflammatory reaction.
A cryo-electron microscopy structure of the virus and its ability to eliminate disseminated tumors in mice were reported on November 25 in Science Translational Medicine.
“The innate immune system is quite efficient at sending viruses to the liver when they are delivered intravenously,” says lead author Dmitry Shayakhmetov, PhD. “For this reason, most oncolytic viruses are delivered directly into the tumor, without affecting metastases. In contrast, we think it will be possible to deliver our modified virus systemically at doses high enough to suppress tumor growth — without triggering life-threatening systemic toxicities.”
In severe cases of COVID-19, Emory researchers have been observing an exuberant activation of B cells, resembling acute flares in systemic lupus erythematosus (SLE), an autoimmune disease.
The findings point towards tests that could separate some COVID-19 patients who need immune-calming therapies from others who may not. It also may begin to explain why some people infected with SARS-CoV-2 produce abundant antibodies against the virus, yet experience poor outcomes.
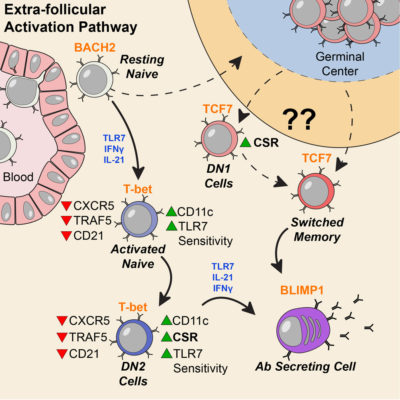
The Emory team’s results converge with recent findings by other investigators, who found that high inflammation in COVID-19 may disrupt the formation of germinal centers, structures in lymph nodes where antibody-producing cells are trained. The Emory group observed that B cell activation is moving ahead along an “extrafollicular” pathway outside germinal centers – looking similar to what they had observed in SLE.
Update: check out first author Matthew Woodruff’s commentary in The Conversation: “The autoimmune-like inflammatory responses my team discovered could simply reflect a ‘normal’ response to a viral infection already out of hand. However, even if this kind of response is ‘normal,’ it doesn’t mean that it’s not dangerous.”
B cells represent a library of blueprints for antibodies, which the immune system can tap to fight infection. In severe COVID-19, the immune system is, in effect, pulling library books off the shelves and throwing them into a disorganized heap.
Before the COVID-19 pandemic, co-senior author Ignacio (Iñaki) Sanz and his lab were focused on studying SLE and how the disease perturbs the development of B cells.
“We came in pretty unbiased,” Sanz says. “It wasn’t until the third or fourth ICU patient whose cells we analyzed, that we realized that we were seeing patterns highly reminiscent of acute flares in SLE.”
In people with SLE, B cells are abnormally activated and avoid the checks and balances that usually constrain them. That often leads to production of “autoantibodies” that react against cells in the body, causing symptoms such as fatigue, joint pain, skin rashes and kidney problems. Flares are times when the symptoms are worse.
In the autoimmune disease systemic lupus erythematosus or SLE, the immune system produces antibodies against parts of the body itself. How cells that produce those antibodies escape the normal “checks and balances” has been unclear, but recent research from Emory University School of Medicine provides information about a missing link.
Investigators led by Ignacio (Iñaki) Sanz, MD, studied blood samples from 90 people living with SLE, focusing on a particular type of B cells. These “DN2” B cells are relatively scarce in healthy people but substantially increased in people with SLE.
The results were published in the journal Immunity.
People with lupus can experience a variety of symptoms, such as fatigue, joint pain, skin rashes and kidney problems. Levels of the DN2 cells were higher in people with more severe disease or kidney problems. DN2 B cells are thought to be “extra-follicular,” which means they are outside the B cell follicles, regions of the lymph nodes where B cells are activated in an immune response.
“Overall, our model is that a lot of lupus auto-antibodies come from a continuous churning out of new responses,” says postdoctoral fellow Scott Jenks, PhD, co-first author of the paper. “There is good evidence that DN2 cells are part of the early B cell activation pathway happening outside B cells’ normal homes in lymph nodes.”
Previous research at Emory has shown that African American women have significantly higher rates of lupus than white women. In the current study, the researchers observed that the frequency of DN2 cells was greater in African American patients. Participants in the study were recruited by Emory, University of Rochester and Johns Hopkins. Read more
People with systemic lupus erythematosus can experience a variety of symptoms, such as fatigue, joint pain, skin rashes and kidney problems. Often the symptoms come and go in episodes called flares. In lupus, the immune system goes haywire and produces antibodies that are directed against the body itself.
A team of Emory scientists has been investigating some fundamental questions about lupus: where do the cells that produce the self-reactive antibodies come from? Are they all the same?
In the accompanying video, Kelli Williams, who helps study the disease and has lupus herself, describes what a flare feels like. In addition, Emory researchers Iñaki Sanz, MD and Chris Tipton, PhD explain their findings, which were published this summer in Nature Immunology.
Judging by the number and breadth of abstracts on lupus at the Department of Medicine Research Day (where Tipton won 1st place for basic science poster), more intriguing findings are in the pipeline. Goofy Star Wars metaphors and more explanations of the science here.
You may have read about recent research, published in Science, describing a technique for revealing which viruses have infected someone by scanning antiviral antibodies in the blood.
Emory immunologists have identified corresponding cells in which long-lived antibody production resides. A subset of plasma cells keep a catalog of how an adult’s immune system responded to infections decades ago, in childhood encounters with measles or mumps viruses.
The results, published Tuesday, July 14 in Immunity, could provide vaccine designers with a goalpost when aiming for long-lasting antibody production.
“If you’re developing a vaccine, you want to fill up this compartment with cells that respond to your target antigen,†says co-senior author F. Eun-Hyung Lee, MD, assistant professor of medicine at Emory University School of Medicine and director of Emory Healthcare’s Asthma, Allergy and Immunology program.
The findings could advance investigation of autoimmune diseases such as lupus erythematosus or rheumatoid arthritis, by better defining the cells that produce auto-reactive antibodies.
Lee says that her team’s research on plasma cells in humans provided insights unavailable from mice, since mice don’t live as long and their plasma cells also have a different pattern of protein markers. More here.